Clinical Vignette
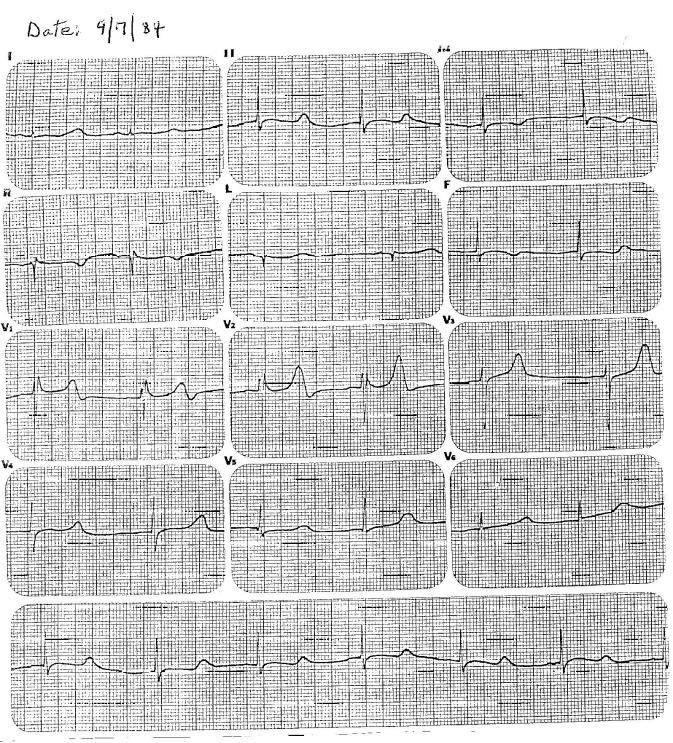
A male patient born in 1968 had an uncomplicated childhood. During early adolescents, he was actively involved in vigorous intramural school sports without symptoms. He experienced a syncopal spell in July 1984 at age 16 when he was watching television at home. He was evaluated by a pediatrician who considered epilepsy as the diagnosis and obtained an electroencephalogram that was normal. No specific therapy was initiated. Two months later, he experienced a second syncopal episode while sitting in class at school. He was evaluated in the Emergency Room of a local hospital. He was not taking any medications or drugs. Exam revealed BP 110/65 mmHg, pulse 50/min, and a soft, grade 2/4 apical systolic murmur with otherwise normal physical and neurological exams. An echocardiogram was obtained and it was interpreted as normal. A 12-lead ECG was obtained on Sept. 7, 1984 (see below).
The ECG is:
ECG Description and Analysis
What is your differential diagnosis, and what do you think is the cause of his two syncopal episodes?
1. Look at V1-V2 repolarization in order to evaluate Brugada Syndrome
2. Measure the QT interval to evaluate LQTS
The ECG is:
Let’s Analyze Case 9
The differential diagnosis for syncope in this age group includes hypertrophic cardiomyopathy,
long QT syndrome, Brugada syndrome, catecholaminergic ventricular tachycardia,
Wolff-Parkinson–White syndrome with transient rapid supraventricular tachycardia,
and coronary artery anomalies with ventricular tachyarrhythmias.
The ECG is diagnostic of long QT syndrome (QT prolongation),
Brugada syndrome (RsR’ with ST elevation in V1-2),
and Wolff-Parkinson-White syndrome (short PR interval, slow initial QRS upstroke, and a wide QRS complex).
Transient cardiac tachyarrhythmias may require Holter monitoring to identify such events.
The echocardiogram is diagnostic of hypertrophic cardiomyopathy with septal hypertrophy and wall-motion abnormalities.
Presently, there are 14 different genetic forms of long QT syndrome,
with LQT1, LQT2 accounting for 80% of the disorders.
LQT3 involves delayed onset of the T wave and accounts for about 7% of patients with long QT syndrome.
The remaining 11 forms of long QT syndrome (LQT4-14) are infrequent
and have been reported mostly in individual families.
The major risk of long QT syndrome is sudden cardiac death.
The diagnosis of long QT syndrome, specifically, LQT3 was evident from the accompanying ECG (HR=50 bpm, QT=0.68 sec, QTc=0.62 sec),
and LQT3 was confirmed by genetic testing.
The patient was treated with a beta-blocker and has remained free of recurrent syncope for more than 30 years.
Family members were checked and his father and two brothers also have long QT syndrome, Type 3 (LQT3).