Clinical Vignette
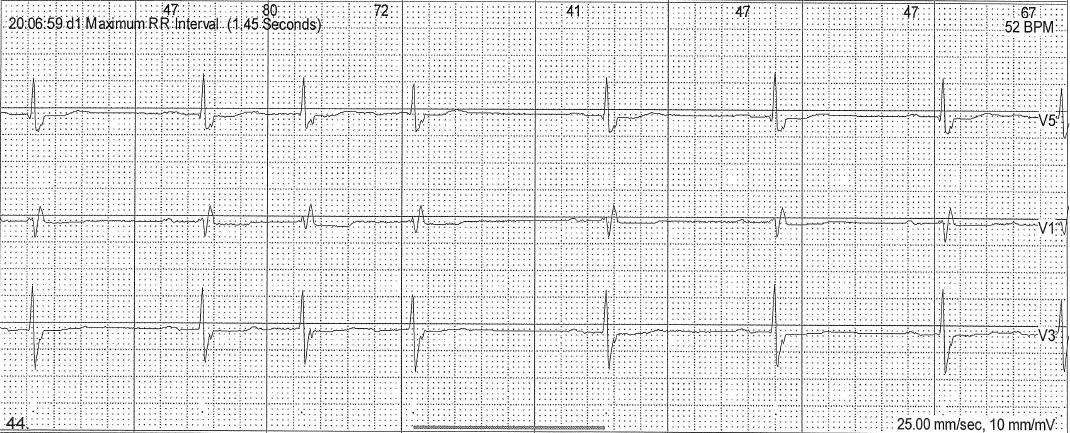
An 88-year-old female with a history of hypertension and paroxysmal atrial fibrillation (AF) was confronted with occasional palpitations without syncope or near-syncope. She is on amiodarone 100 mg 5 days a week. A 24-hour Holter monitor was obtained for the evaluation of the palpitations. Selected tracings from the Holter recording are shown.
The ECG is:
What’s Your Diagnosis?
Pseudo-ventricular tachycardia (VT) is defined as a wide complex tachycardia mimicking VT. Pseudo-VT, like true VT, poses similar concerns to the physicians, nurses, and technicians and results in misinterpretation and adverse outcomes due to inappropriate diagnosis and management.
It is almost always due to artifacts such as loose electrodes, tremors, patient motion, epilepsy, electrical and device interference.
Here, we present two cases that are due to loose electrodes (case 1) and electrical interference, respectively (case 2).
Pseudo-VT may be confusing and can result in an inappropriate diagnosis and management. Here are some clues to avoid misdiagnosis and mismanagement:
1. Keep the diagnosis in mind
2. Measure the intervals, and if the patient carries any electronic devices such as pacemaker, implantable cardioverter-defibrillator, left ventricular assist device, etc., consider electrical interference with other devices.
3. Look at all leads, and if the patient carries a pacemaker, ICD or CRT, interrogate the devices and measure all intracardiac intervals and markers.
4. Correlate with patient symptoms as they are almost always artifact. Patients remain asymptomatic unless the pseudo-VT triggers the device, which delivers a shock. Correct diagnosis will avoid unnecessary steps and procedures.
5. Look at previous ECGs. Compared to previous ECGs, if the patient is stable, no urgent steps are needed.
ECG criteria/clues on how to differentiate pseudo-VT from real VT:
1. ECG characteristics of real VT are often not present in pseudo-VT.
2. Sinus rhythm or underlying rhythm is often present in one of the leads (Figure).[3]
3. Presence of “notch” sign in a pseudo-VT tracing that are produced by the underlying rhythm is highly suggestive of pseudo-VT (see figure 2-4, arrows).[4]
4. Clinically, patients with pseudo-VT are almost always asymptomatic and hemodynamically stable.
Accurate analysis of ECGs by comparing it with previous ones as well as analysis of intracardiac electrograms and event monitors often leads to the correct diagnosis of “artifact” and avoids inappropriate diagnosis and management steps. The most common cause of inappropriate ICD discharges are body tremors.
In patients with cardiac rhythm management devices, the most common causes of inappropriate ICD shocks are:
1. Misprogramming and misdetection of native rhythms
2. Lead defect and fraction
3. External electrical interference
4. Patient motion and tremor