Clinical Vignette
A 27-year old woman is referred for consultation because of the presence of a systolic murmur.
The ECG is:

ECG Description and Analysis
Please perform a systematic analysis of the 12-lead ECG.
1. QRS axis in the frontal plane?
2. Is the R wave height in the precordial leads normal?
3. What about the R/S ratio in the precordial leads?
The ECG is:
Let’s Analyze Case 10
What is the rhythm? A P wave precedes the QRS complexes with a constant and normal PR interval, and the P wave is positive in both I and aVF, indicating sinus rhythm with normal P wave axis.
In terms of frontal plane QRS axis, a predominantly positive QRS complex in II, III (with tallest R wave) and aVF, while aVR shows equal positive and negative amplitudes indicate that the axis is in the right inferior quadrant, or +120°.
The QRS duration is <120 ms. The ventricular activation time or R wave peak time in the right precordial leads is >30 ms. The QRS complex reveals a qR/qRs in V4R and V1. The presence of an initial q wave in V1 is indicative of supra-systemic right ventricular pressure overload.
The phenomenon is explained by the prominent right ventricle: the interventricular septum would be approximately parallel to the frontal plane, and the first vector (activation of the mid-septum), by the extreme rotation of the heart around the longitudinal axis, is now oriented to the left, producing a small initial q wave in V1 and tall R waves in V1-V3 (prominent anterior forces).
In addition, the R/S ratio in the precordial leads is positive in all leads, with no transition zone. There is ST depression, convex upward, followed by a negative T wave in II, III, aVF, and V1-V5 suggesting a right ventricular strain pattern. The QT interval is normal at 440 ms.
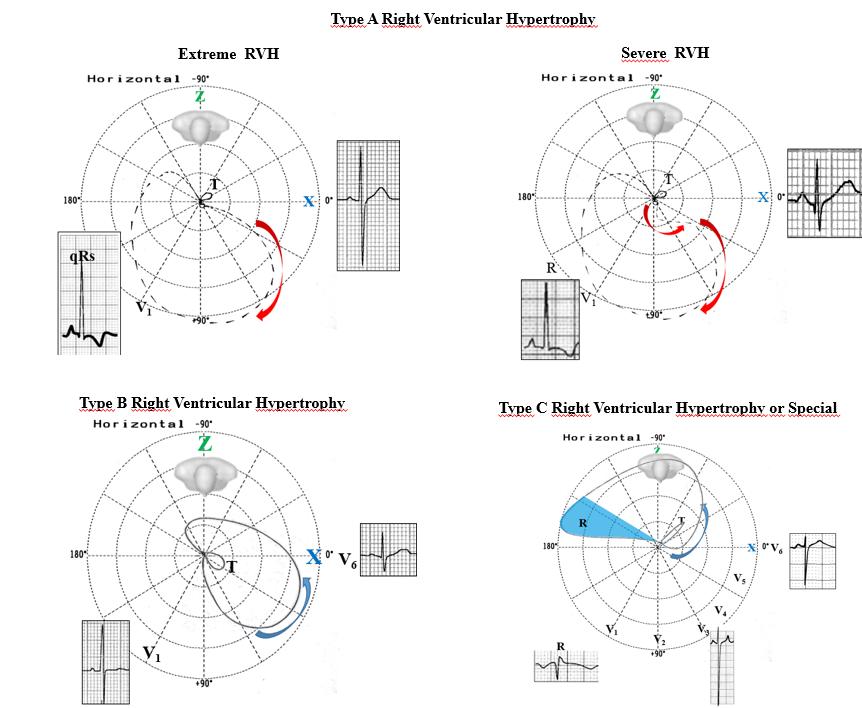
RVH type A: QRS loop with clockwise rotation and axis predominantly located in the anterior right quadrant. Typical of RVH in congenital heart disease with severe right ventricular pressure overload.
RVH type B: QRS loop with counter-clockwise rotation predominantly located in the anterior right or left quadrant. Typical of moderately severe RVH.
RVH type C: Typical of emphysema. QRS loop with counter-clockwise rotation predominantly located in the right posterior quadrant.