Clinical Vignette
An 88-year-old woman presents with chest pain worsened by breathing and movement.
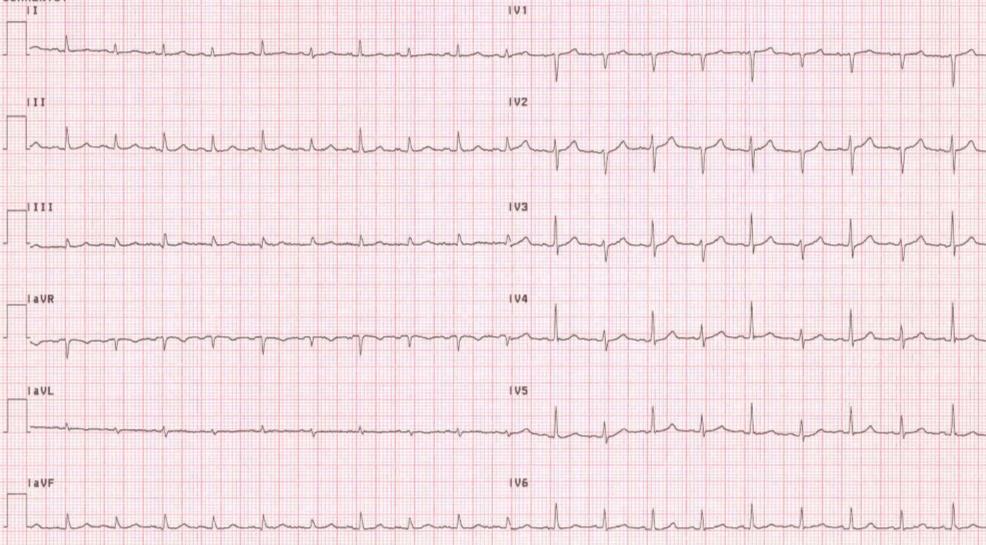
This ECG is characterized by 2 important abnormalities:
1. ST segment elevation, and
2. PR segment depression.
The ECG is:
ECG Description and Analysis
This ECG is characterized by 2 important abnormalities:
1. ST segment elevation, and
2. PR segment depression.
The ECG is:
Let’s Analyze Case 7
1. ST segment elevation
The ST segment elevation is due to epicardial injury as may be seen in transmural ischemia or pericardial injury.
Notably, the ST segment elevation is widespread and is not in keeping with the distribution of a single coronary artery,
as would be expected in transmural ischemia.
In addition, there is no reciprocal ST depression in any of the epicardial leads.
ST depression is only seen in lead aVR which looks primarily at the endocardium.
These findings suggest that the injury current is diffuse and epicardial only. Typically, in transmural ischemia due to acute myocardial infarction the pattern of epicardial injury is limited to the myocardium at risk due to the occlusion of the culprit coronary artery. Areas of the myocardium at a distance from the acute infarction may demonstrate reciprocal ST segment depression as the current of injury (ST segment elevation) is not seen in those areas. Myocardium at a distance should not, however, demonstrate ST segment elevation. Lead aVR and (sometimes V1) are viewing primarily endocardial activation and for that reason typically show ST depression in cases of pericarditis. The concave upward appearance of the ST segment, as seen here, is typical of pericarditis, but may also be seen in ischemic injury, so should not be relied upon as a sole criterion for pericarditis.
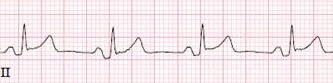
2. PR segment depression
PR segment depression is best seen here below in the magnified portion of Lead II from the ECG above.
Extension of a horizontal line along the baseline (TP segment) clearly demonstrates that the PR segment falls below the baseline (arrows).
This is due to the fact that the pericardium reflects over the atria as well as the ventricles
and thus may cause atrial repolarization injury (PR segment depression).
Other points of differentiation from ischemic ST segment elevation.
Typically in ischemic injury there is evidence of changes in the QRS complex due to myocardial infarction.
This becomes especially true after some time has passed but is often seen immediately.
Pericarditis does not typically affect the QRS complex.
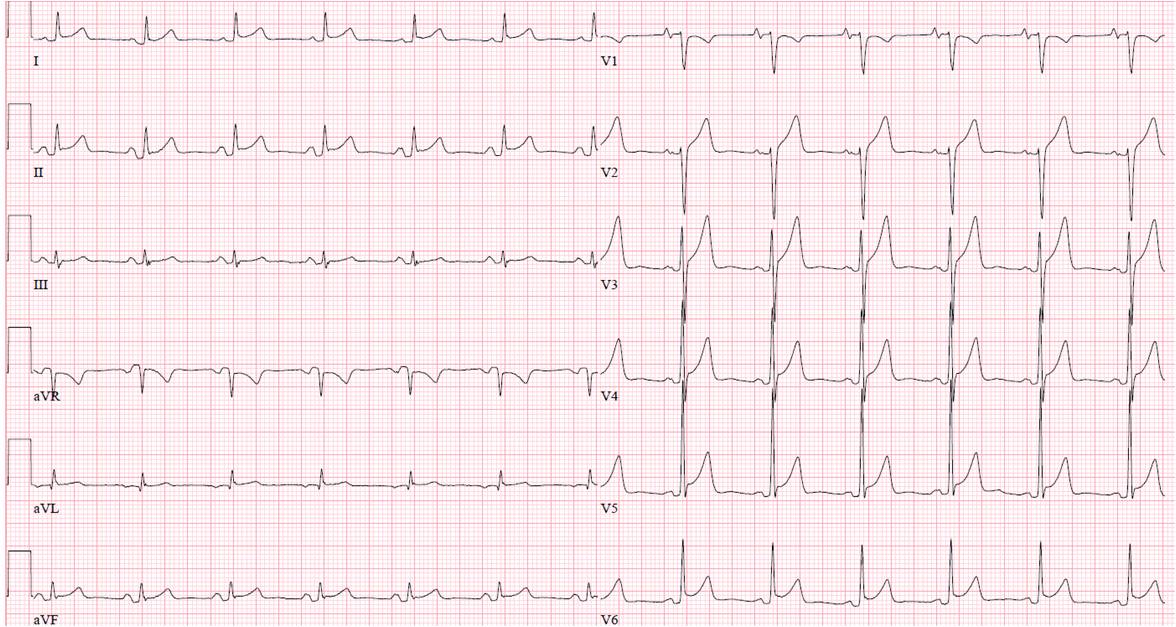
Special Situations in Pericarditis.
Occasionally, as seen below in this ECG from a 28-year-old man presenting with dyspnea,
there may be sinus tachycardia associated with QRS alternans.
This is associated with a large, usually malignant, pericardial effusion
due to the swinging of the heart within the fluid-filled pericardial sac.