Let’s Analyze Case 5
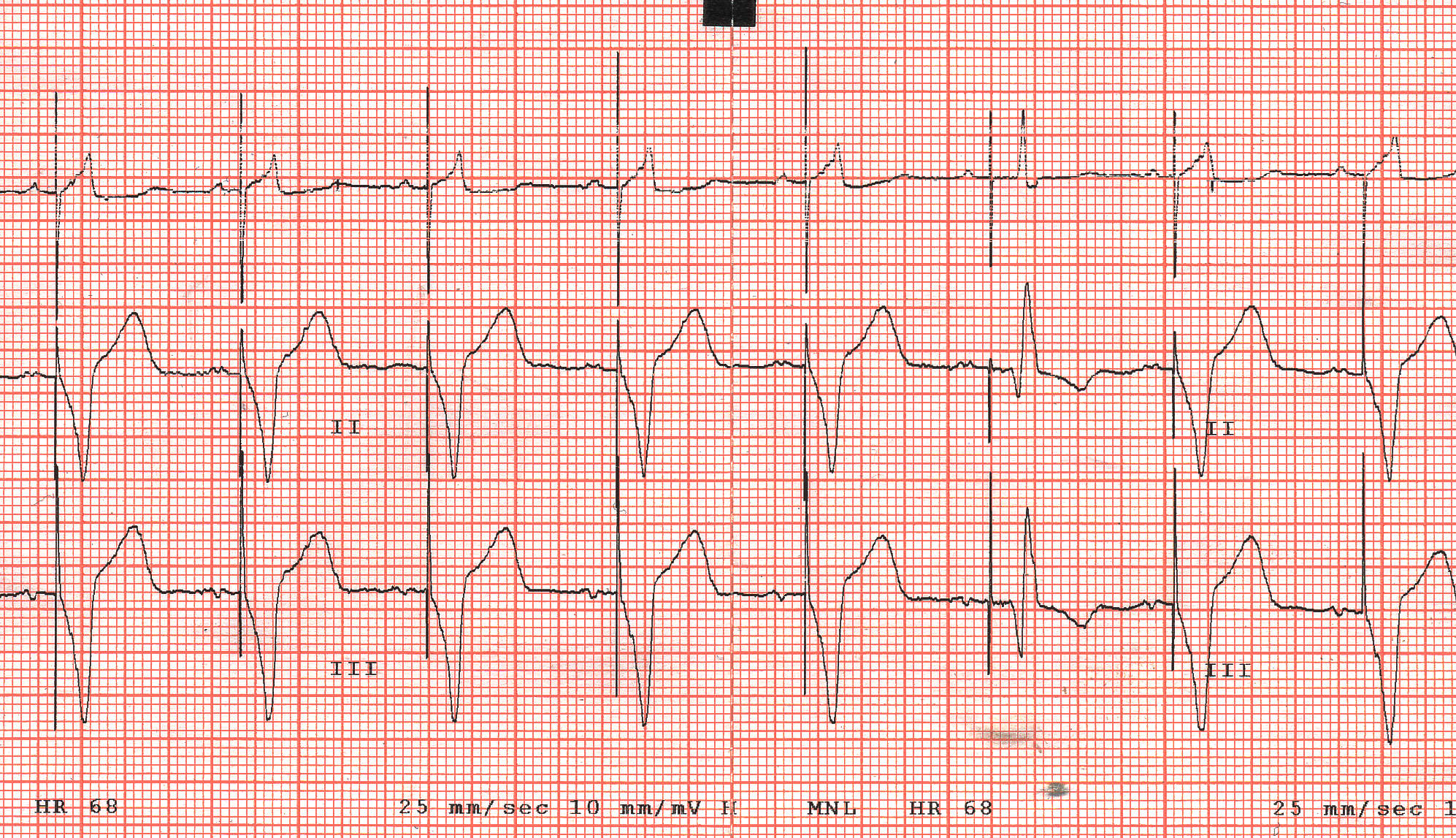
The first five cardiac evolutions are the same, they start with a p wave, positive in leads I and II and occurring at a rate of 68 bpm.
This is strongly suggestive of a normal sinus rhythm.
Each p wave is followed by a pacing artifact/spike.
The interval between p wave and the pacing spike is constant (approximately 180 ms), mimicking normal atrioventricular conduction.
After each pacing spike there is a QRS complex.
Together, this is a typical ECG appearance of cardiac pacing in the ventricles synchronized to the atrial activity, i.e., of a dual chamber pacing.
Since there is no evidence of pacing in the atrium, this might be either a DDD pacemaker (most common variety) or a VDD pacemaker.
The key observation in the current tracing is the sixth cardiac evolution that is different in two aspects from all other evolutions.
Firstly, the QRS complex is narrower.
Secondly, the pacing spike is not immediately followed by a QRS complex but there is an 80 ms isoelectric interval between the pacing spike and the QRS.
If the pacing spike is not immediately followed by a myocardial response, i.e., either by a p wave or a QRS complex, it is almost diagnostic of failure to capture.
There are only two rare possibilities when there can be an isoelectric interval after the pacing spike without failure to capture being present:
1. A phenomenon known as latency.
2. Direct, selective His bundle capture.
Both can be easily excluded in the current case.
Since the ventricles are not captured, why is there a QRS complex present at all?
The answer is simple: this is an intrinsic, conducted QRS complex, albeit with a first degree atrioventricular block (PR interval of 280 ms).
Exercise Based on Case 5
1. What are the most common causes of failure to capture?
2. Since most pacing spikes capture the ventricle, is this a serious pacemaker failure requiring urgent reprogramming/system revision or can this wait until planned, routine pacemaker follow-up?
3. Is the morphology of the paced QRS complexes suggestive of pacing lead position?
4. Does the morphology of the intrinsic QRS complex reveal the underlying heart disease?
What’s Your Diagnosis?
This is ventricular pacing in VDD mode with occasional failure to capture the ventricles. In a patient with atrioventricular block, this is an ominous finding, a warning sign that a symptomatic bradyasystolic event is around the corner.