Clinical Vignette
The importance of clinical and history and previous ECG tracings in the clinical interpretation of a patient with LAFB and syncope.
Male patient, aged 70yrs, recent history of unexplained syncope, intraventricular conduction delay on ECG at ER.
The ECG is:
ECG Description and Analysis
In tracings with intraventricular conduction disturbances, three questions should be formulated:
1. What is the QRS axis?
2. What is the QRS duration?
3. What is the cycle length duration?
The ECG is:
Let’s Analyze Case 2
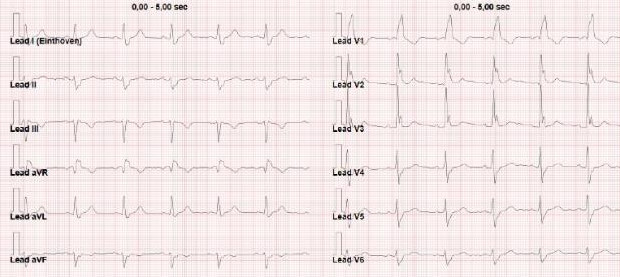
The ECG on admission (Figure 1) shows a bifascicular block, with left anterior fascicular block (LAFB) and right bundle branch block (RBBB) with QRS duration 160 msec and QRS axis -30°.
From the Hospital ECG data bank, it was possible to retrieve a previous tracing of this patient:
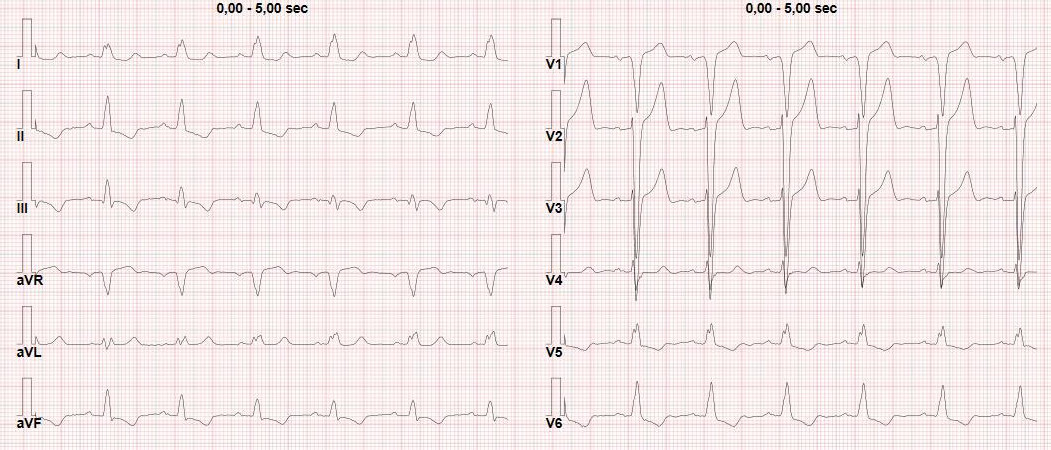
The previous ECG showed left bundle branch block (LBBB), with LAFB and left posterior fascicular block (LPFB), with QRS duration 140 msec and QRS axis 45° (at that time the patient was asymptomatic).
The comparison of the two tracings suggests a possible interpretation of this case:
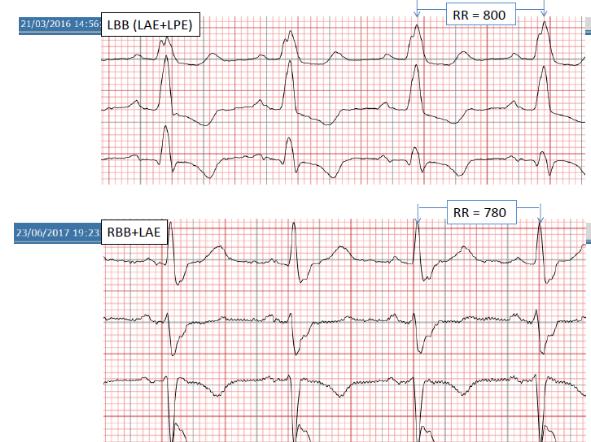
Upper tracing (2016): In presence of LBBB, i.e. complete block of both LAF and LPF, with a QRS duration of 140 msec, the activation of Purkinje fibers occurs by the RBB.
Lower tracing (2017): In presence of RBBB+LAFB, the activation of the Purkinje fibers occurs by the left posterior fascicular branch (LPF), with a QRS duration 160 msec.
As the RBB worsens its conduction, the impulse is only conducted along the LPF, already known to be delayed, therefore the syncope is probably due to a transient LPFB, giving rise to a trifascicular block.