Clinical Vignette
A 76-year old man who have ever experienced a fainting.
The ECG is:
ECG Description and Analysis
In this 12-lead ECG, three questions should be formulated:
1. Is ECG axis normal in the limb leads?
2. Is QRS configuration or duration normal in the precordial leads?
3. What happened to the conduction system?
The ECG is:
Let’s Analyze Case 12
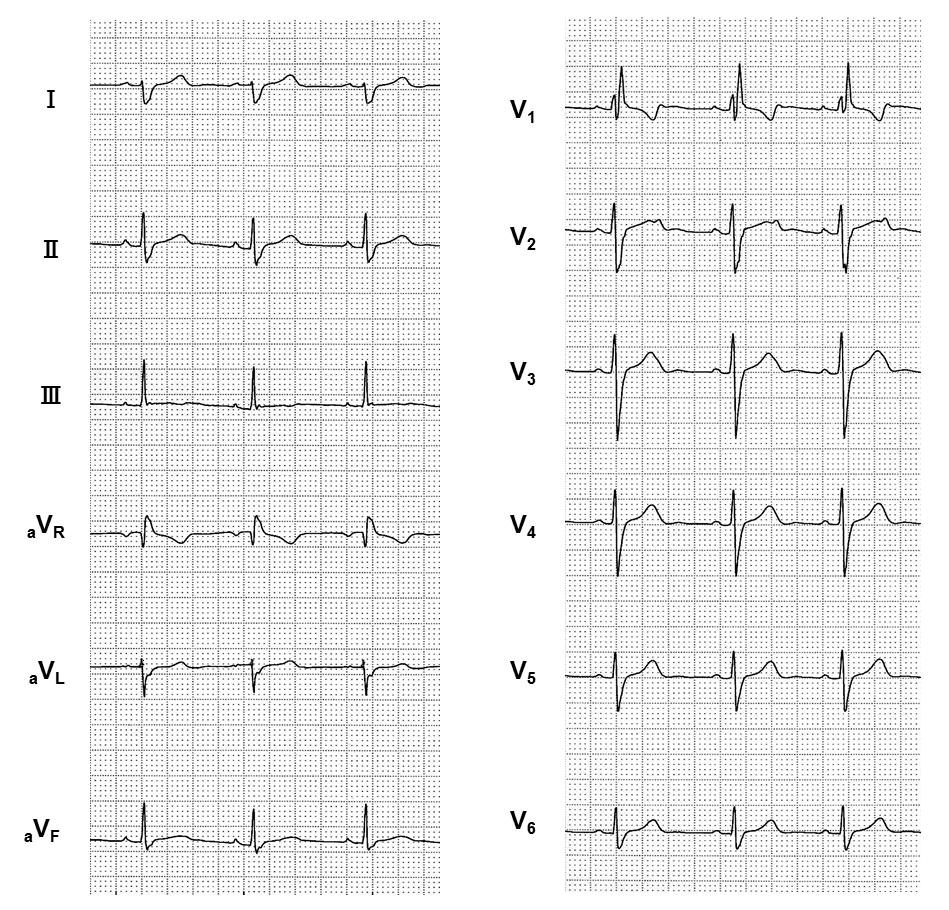
Normal QRS axis in the limb leads is between -30° and +90°. When the axis is greater than +90°, it is determined as right axis deviation (RAD).
In this case, apparent small R waves with deep S waves (= rS pattern) in leads I and aVL are observed.
This pattern is consistent with diagnostic ECG criteria for left posterior fascicular block (LPFB).
QRS durations in the limb leads are slightly prolonged.
This pattern is also compatible with findings of LPFB because LPFB in isolation is extremely rare and in most cases LPFB is accompanied by right bundle branch block (RBBB).
Wide QRS complexes >120 ms are seen in the precordial leads.
RSR’ pattern (‘M-shaped’ QRS complex) in lead V1 and wide, slurred S waves in the lateral leads (I, aVL, V5-V6) are observed.
This pattern is consistent with diagnostic ECG criteria for RBBB.
In conclusion, this case represents LPFB accompanied by RBBB (bifascicular block).
When LPFB is present in isolation, small q waves with tall R waves (= qR pattern) may be seen in the inferior leads (II, III, and aVF), but this finding is quite rare as mentioned above.
For diagnosis of LPFB, it is important that more significant causes of RAD such as right ventricular hypertrophy, pulmonary hypertension, and pulmonary embolism have to be ruled out
because LPFB is defined as absence of any other causes for RAD.
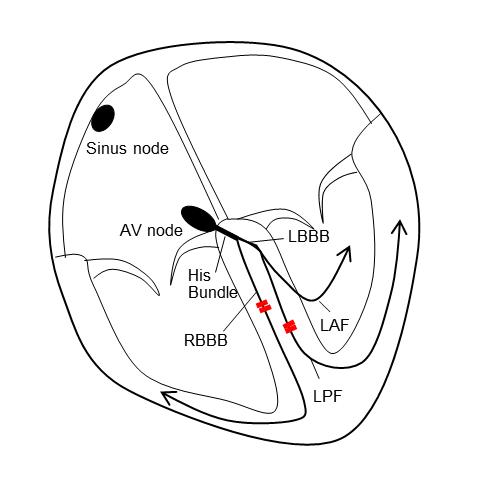
Bifascicular block is defined as the combination of RBBB with either left anterior fascicular block (LAFB) or LPFB.
Conduction to the ventricles is via the single remaining fascicle.
In this case, it is the left anterior fascicle (Fig. 1).
Although LAFB is often observed in 12-lead ECG even in healthy subjects as well as RBBB, LPFB is much less common than LAFB and RBBB
because the left posterior fascicle is a broad bundle of fibers and resistant to damage.
Thus, RBBB + LAFB is the more common of the two patterns, but RBBB + LPFB is rare.
Management and Therapeutic Considerations
Bifascicular block due to the combination of RBBB and LPFB is a sign of extensive conducting system disease such as complete heart block.
This patient was followed with an implantable loop recorder (ILR).
Two months later, paroxysmal atrioventricular block was recorded on the ILR showing cardiac arrest of 13 seconds.
At that time, the patient had syncope. Eventually, a pacemaker (DDD mode) was implanted.