Clinical Vignette
74 year old asymptomatic male with a history of hypertension (treated with ACE and hydralazine) noted to have bradycardia.
The ECG is:
ECG Description and Analysis
1. Is this an atrial tachycardia, flutter or fibrillation?2. Is there a relationship between atria and ventricle activation?
3. Is there complete heart block?
The ECG is:
Let’s analyze Case 13
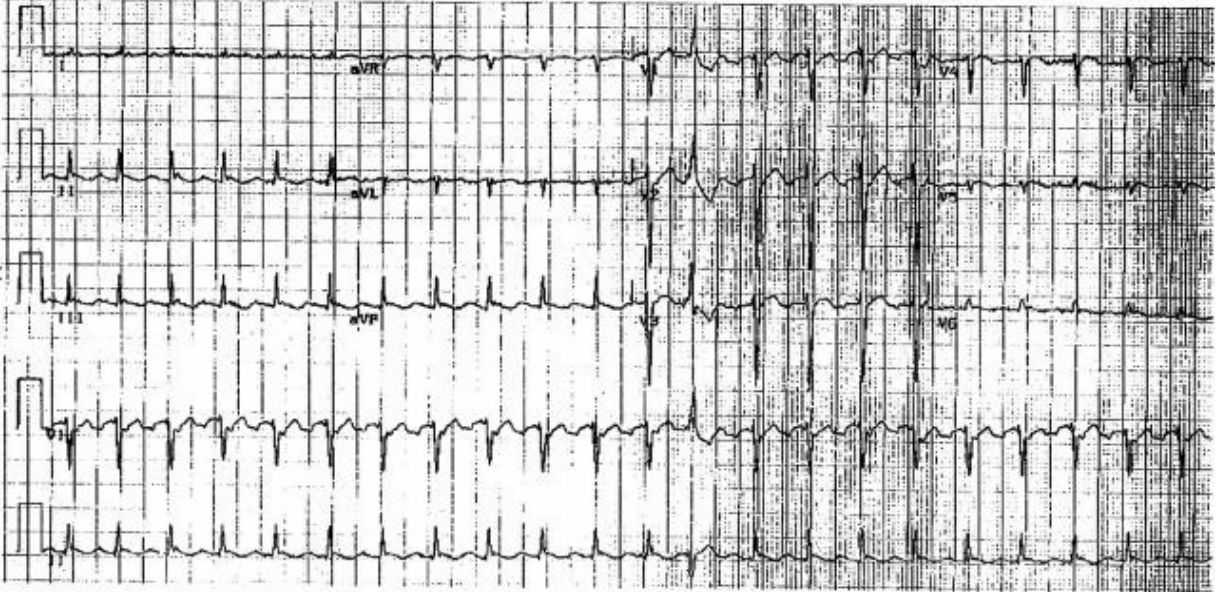
The P (or “f”) waves are regular and rapid (CL 240 ms) with a “sawtooth” pattern in inferior leads, and small amplitude positive polarity waves in V1.
This pattern is characteristic of counterclockwise atrial flutter.
Notably, the ventricular activation is irregular with bradycardia (<50 bpm).
Typical “counterclockwise” atrial flutter results from a right atrial re-entrant circuit.
The wavefront propagates up the atrial septum, across the superior aspect of the chamber, then inferiorly down the right atrial free wall to re-enter the atrial septum.
(Although classically regarded as following the tricuspid ring, recent data indicate that the margins of the driving circuit may be variable [Santucci et al]).
The 12-lead ECG during typical atrial flutter with characteristic negative “sawtooth” atrial flutter waves in leads II, III, and aVF is generated by the pattern of left atrial depolarization [Okumara et al].
Less commonly, the impulse may travel in the opposite direction, i.e., reverse typical atrial flutter (the term atypical atrial flutter should be avoided).
AV conduction typically occurs with even levels of AV block, e.g., 2:1, 4:1, etc.
Irregular conduction may imply concomitant drug therapy with AV nodal blocking agents or intrinsic AV nodal disease.
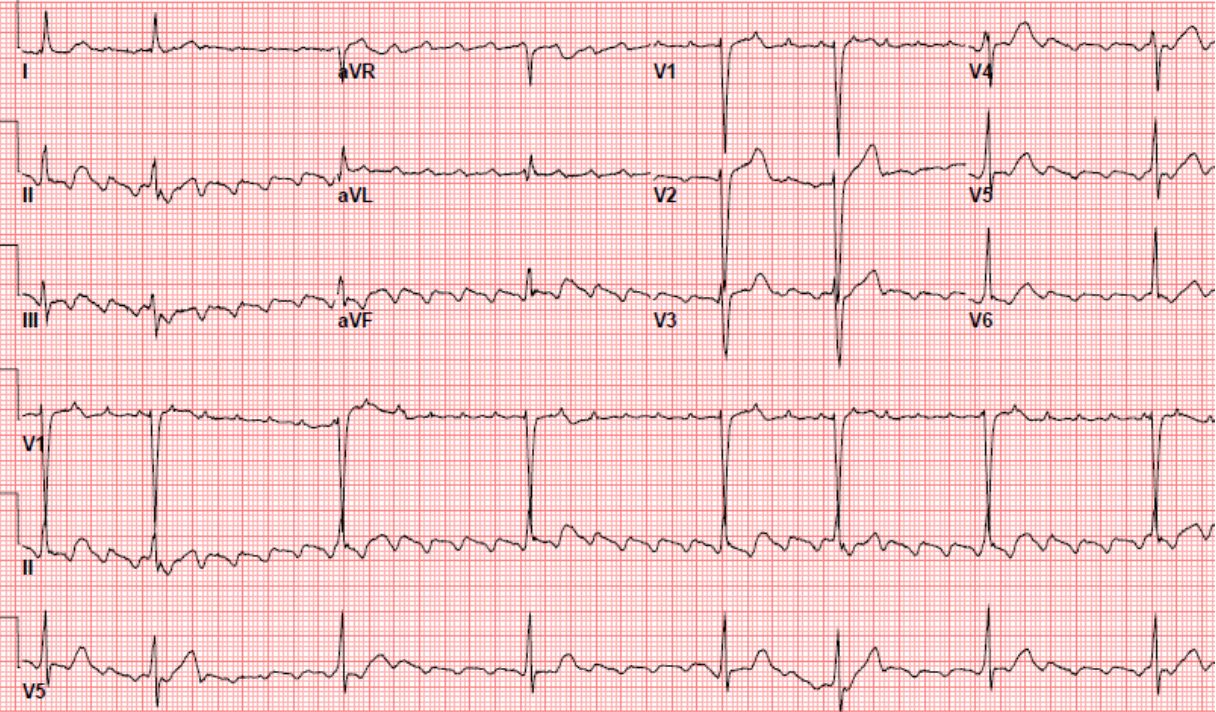
In this case, reversion to sinus rhythm showed Wenckebach with the shortest PR interval of 360 ms indicative of underlying conduction system disease in this individual.
Presentation
Atrial flutter may present paroxysmally or as a persistent arrhythmia.
Conduction with rapid ventricular rate is responsible for many of the associated symptoms, e.g., palpitations or dizziness.
(In this case, the well-controlled ventricular response likely accounted for asymptomatic status).
The alternative explanation for dizziness is from post-conversion pauses– late recovery of sinus node activity following spontaneous termination of flutter generates offset pauses.
This is common since patients with atrial flutter have sinus node dysfunction (sick sinus syndrome).
Treatment
Anticoagulation should be used in the same fashion as for AF.
Pharmacotherapy for sinus rhythm retention or ventricular rate control is often ineffective and/or poorly tolerated.
Catheter ablation is preferred [Natale], targeting the isthmus bounded by the inferior vena cava, Eustachian ridge,
the coronary sinus os on one side, and the tricuspid valve annulus on the other side (the “atrial flutter isthmus”).
Follow Up
Since atrial flutter often coexists with atrial fibrillation, it is important to monitor for the emergence of AF following successful treatment of flutter.